

INTRODUCTION
BACKGROUND
The prevalence of folic acid deficiency has decreased since the United States and Canada introduced a mandatory folic acid food fortification program in November 1998. People with excessive alcohol intake and malnutrition are still at high risk of folic acid deficiency.
Figure 4.
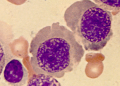
Histologically, the megaloblastosis caused by folic acid deficiency cannot be differentiated from that observed with vitamin B-12 deficiency.
The significance of folic acid deficiency is compounded further by the following attributes:
An association of folate deficiency with elevated homocysteine, leading to increased arteriosclerosis risks. The reduced incidence of neural tube defects with folate supplementationThe role of folate in the occurrence of cancer
Hence, folic acid clearly is of consequence in public health in the United States, especially because heart disease and cancer constitute the number 1 and number 2 causes of mortality in the United States. This article explores the mechanisms and manifestations behind folate deficiency, as well as its ramifications with regard to health and disease at large.
PATHOPHYSIOLOGY
Folic acid is composed of a pterin ring connected to p-aminobenzoic acid (PABA) and conjugated with one or more glutamate residues. It is distributed widely in green leafy vegetables, citrus fruits, and animal products. Humans do not generate folate endogenously because they cannot synthesize PABA, nor can they conjugate the first glutamate.
Folates are present in natural foods and tissues as polyglutamates because these forms serve to keep the folates within cells. In plasma and urine, they are found as monoglutamates because this is the only form that can be transported across membranes. Enzymes in the lumen of the small intestine convert the polyglutamate form to the monoglutamate form of the folate, which is absorbed in the proximal jejunum via both active and passive transport.
Within the plasma, folate is present, mostly in the 5-methyltetrahydrofolate (5-methyl THFA) form, and is loosely associated with plasma albumin in circulation. The 5-methyl THFA enters the cell via a diverse range of folate transporters with differing affinities and mechanisms (ie, adenosine triphosphate [ATP]–dependent H+ cotransporter or anion exchanger). Once inside, 5-methyl THFA may be demethylated to THFA, the active form participating in folate-dependent enzymatic reactions. Cobalamin (B-12) is required in this conversion, and in its absence, folate is "trapped" as 5-methyl THFA.
From then on, folate no longer is able to participate in its metabolic pathways, and megaloblastic anemia results. Large doses of supplemental folate can bypass the folate trap, and megaloblastic anemia will not occur. However, the neurologic/psychiatric abnormalities associated with B-12 deficiency ensue progressively.
The biologically active form of folic acid is tetrahydrofolic acid (THFA), which is derived by the 2-step reduction of folate involving dihydrofolate reductase. THFA plays a key role in the transfer of 1-carbon units (such as methyl, methylene, and formyl groups) to the essential substrates involved in the synthesis of DNA, RNA, and proteins. More specifically, THFA is involved with the enzymatic reactions necessary to synthesis of purine, thymidine, and amino acid. Manifestations of folate deficiency thereafter, not surprisingly, would involve impairment of cell division, accumulation of possibly toxic metabolites such as homocysteine, and impairment of methylation reactions involved in the regulation of gene expression, thus increasing neoplastic risks.
A healthy individual has about 500-20,000 mcg of folate in body stores. Humans need to absorb approximately 50-100 mcg of folate per day in order to replenish the daily degradation and loss through urine and bile. Otherwise, signs and symptoms of deficiency can manifest after 4 months.
EPIDEMIOLOGY
Frequency
United States
The current standard of practice is that serum folate levels less than 3 ng/mL and a red blood cell (RBC) folate level less than 140 ng/mL puts an individual at high risk of folate deficiency. The RBC folate level generally indicates folate stored in the body, whereas the serum folate level tends to reflect acute changes in folate intake.
Data from the National Health and Nutrition Examination Survey (NHANES) 1999-2016 indicate the prevalence of low serum folate concentrations (< 6.8 nmol/L) decreased from 16% before folic acid fortification to 0.5% after folic acid fortification.
The folate insufficiency prevalence (RBC folate <748 nmol/L; NTD risk) in women decreased from 2007–2010 (23.2%) to 2011–2016 (18.6%) overall. The prevalence of folate insufficiency (risk of NTDs) in women of reproductive age decreased from 59% prefortification (1988–1994) to 15% (1999–2006) and 23% (2007–2010) postfortification.
In elderly persons, the prevalence of high serum folate concentrations (>45.3 not/L) increased from 7% before fortification to 38% after fortification.
International
Countries that do not have a mandatory folic acid food fortification program have higher rates of folic acid deficiency. For example, a population based study in Iran (where there is no fortification) showed an age-adjusted prevalence of hyperhomocysteinemia (Hcy >15 micromol/L) of 73.1% in men and 41.07% in women (aged 25-64 y).
Casey et al examined the effects over 1 year of a free weekly iron-folic acid supplementation and deworming program in 52,000 Vietnamese women of childbearing age. The investigators collected demographic data and blood and stool samples at baseline and at 3 and 12 months following the implementation of the program.
Findings included a mean Hb increase of 9.6 g/L (P< 0.001) and a reduction in the presence of anemia from 37.5% of the women at baseline to 19.3% at 12 months. Iron deficiency was also reduced, from 22.8% at baseline to 9.3% by 12 months, as well as hookworm infection (76.2% at baseline to 23.0%) in the same period.
A discussion of selected national Australian policies is presented in Lawrence et al.[5]
Mortality/Morbidity
Hematologic Manifestations
Folate deficiency can cause anemia. The presentation typically consists of macrocytosis and hypersegmented polymorphonuclear leucocytes (PMNs). More detailed laboratory findings are discussed in the Workup section.
The anemia usually progresses over several months, and the patient typically does not express symptoms as such until the hematocrit level reaches less than 20%. At that point, symptoms such as weakness, fatigue, difficulty concentrating, irritability, headache, palpitations, and shortness of breath can occur. Furthermore, heart failure can develop in light of high-output cardiac compensation for the decreased tissue oxygenation. Angina pectoris may occur in predisposed individuals due to increased cardiac work demand. Tachycardia, postural hypotension, and lactic acidosis are other common findings. Less commonly, neutropenia and thrombocytopenia also will occur, although it usually will not be as severe as the anemia. In rare cases, the absolute neutrophil count can drop below 1000/mL and the platelet count below 50,000/mL.
Elevated Serum Homocysteine and Atherosclerosis
Folate in the 5-methyl THFA form is a cosubstrate required by methionine synthase when it converts homocysteine to methionine. As a result, in the scenario of folate deficiency, homocysteine accumulates. Several recent clinical studies have indicated that mild-to-moderate hyperhomocystinemia is highly associated with atherosclerotic vascular disease such as coronary artery disease (CAD) and stroke. In this case, mild hyperhomocystinemia is defined as total plasma concentration of 15-25 mmol/L and moderate hyperhomocystinemia is defined as 26-50 mmol/L.
Genest et al found that a group of 170 men with premature coronary artery disease had a significantly higher average level of homocysteine (13.7 ± 6.4). In another study, Coull et al found that among 99 patients with stroke or transient ischemic attacks (TIAs), about one third had elevated homocysteine.
Elevated homocysteine levels might act as an atherogenic factor by converting a stable plaque into an unstable, potentially occlusive, lesion. Wang et al found that in patients with acute coronary syndromes, levels of homocysteine and monocyte chemoattractant protein-1 (MCP-1) were significantly higher. MCP-1 is a chemokine characterized by the ability to induce migration and activation of monocytes and therefore may contribute to the pathogenesis of CAD. Homocysteine is believed to have atherogenic and prothrombotic properties via multiple mechanisms.
Bokhari et al found that among patients with CAD, the homocysteine level correlates independently with left ventricular systolic function. The mechanism is unknown, but it may be due to a direct toxic effect of homocysteine on myocardial function separate from its effect on coronary atherosclerosis.
Although in multiple observational studies elevated plasma homocysteine levels have been positively associated with increased risk of atherosclerosis, randomized trials have not been able to demonstrate the utility of homocysteine-lowering therapy. In the Heart Outcomes Prevention Evaluation (HOPE) 2 trial, supplements combining folic acid and vitamins B6 and B12 did not reduce the risk of major cardiovascular events in patients with vascular disease. Similarly, in the trial of Bonaa et al treatment with B vitamins did not lower the risk of recurrent cardiovascular disease after acute myocardial infarction.
Pregnancy Complications
Possible pregnancy complications secondary to maternal folate status may include spontaneous abortion, abruption placentae, and congenital malformations (eg, neural tube defect). In a literature review, Ray et al examined 8 studies that demonstrated association between hyperhomocystinemia and placental abruption/infarction. Folate deficiency also was a risk factor for placental abruption/infarction, although less statistically significant.
Several observational and controlled trials have shown that neural tube defects can be reduced by 80% or more when folic acid supplementation is started before conception. In countries like the United States and Canada, the policy of widespread fortification of flour with folic acid has proved effective in reducing the number of neural tube defects.
Although the exact mechanism is not understood, a relative folate shortage may exacerbate an underlying genetic predisposition to neural tube defects.
Effects on Carcinogens
Diminished folate status is associated with enhanced carcinogenesis. A number of epidemiologic and case-control studies have shown that folic acid intake is inversely related to colon cancer risk. With regard to the underlying mechanism, Blount et al showed that folate deficiency can cause a massive incorporation of uracil into human DNA leading to chromosome breaks. Another study by Kim et al suggested that folate deficiency induces DNA strand breaks and hypomethylation within the p53 gene.
Effects on Cognitive Function
Several studies have shown that an elevated homocysteine level correlates with cognitive decline. In Herbert's classic study in which a human subject (himself) was in induced folate deficiency from diet restriction, he noted that CNS effects, including irritability, forgetfulness, and progressive sleeplessness, appeared within 4-5 months. Interestingly, all CNS symptoms were reported to disappear within 48 hours after oral folate intake.
Low folate and high homocysteine levels are a risk factor for cognitive decline in high-functioning older adults and high homocysteine level is an independent predictor of cognitive impairment among long-term stay geriatric patients.
Mechanistically speaking, current theory proposes that folate is essential for synthesis of S-adenosylmethionine, which is involved in numerous methylation reactions. This methylation process is central to the biochemical basis of proper neuropsychiatric functioning.
Despite the association of high homocysteine level and poor cognitive function, homocysteine-lowering therapy using supplementation with vitamins B-12 and B-6 was not associated with improved cognitive performance after two years in a double-blind, randomized trial in healthy older adults with elevated homocysteine levels.
Sex
Women who are pregnant are at higher risk of developing folate deficiency because of increased requirements.
Age
Elderly people also may be more susceptible to folate deficiency in light of their predisposition to mental status changes, social isolation, low intake of leafy vegetables and fruits, malnutrition, and comorbid medical conditions. The greatest risk appears to be among low-income populations and institutionalized elderly people and less risk among the free-living elderly population.

